Abstract Interventions to address the U.S. opioid crisis primarily target opioid use, misuse, & addiction, but because the opioid crisis includes multiple substances, the opioid specificity of interventions may limit their ability to address the broader problem of polysubstance use. Overlap of opioids with other substances ranges from shifts among the substances used across the lifespan to simultaneous co-use of substances that span similar & disparate pharmacological categories. Evidence suggests that nonmedical opioid users quite commonly use other drugs, & this polysubstance use contributes to increased morbidity & mortality. Reasons for adding other substances to opioids include enhancement of the high (additive or synergistic reward), compensation for undesired effects of one drug by taking another, compensation for negative internal states, or a common predisposition that is related to all substance consumption. But consumption of multiple substances may itself have unique effects. To achieve the maximum benefit, addressing the overlap of opioids with multiple other substances is needed across the spectrum of prevention & treatment interventions, overdose reversal, public health surveillance, & research. By addressing the multiple patterns of consumption and the reasons that people mix opioids with other substances, interventions & research may be enhanced.
Introduction The U.S. opioid crisis exerts a major impact on health & social outcomes. Since 2005, deaths due to opioid overdoses exceed 500,000, & declines in overall U.S. life expectancy are at least partly explained by overdose mortality Morbidity caused by opioids includes increasing infectious disease (particularly HIV, hepatitis, and endocarditis), sleep disorders, affective disorders, and increasing neonatal opioid withdrawal, among other outcomes. The overall economic impact of opioid misuse was estimated at $500 billion per year in 2017.
In response, prevention & treatment practices and policies have been implemented widely. These include expanding access to medications for opioid use disorder (OUD), reducing opioid prescribing, increasing access to naloxone, improving public health surveillance, increasing access to harm reduction programs such as syringe services, & major investments in research. All of these interventions target opioid use, misuse, and addiction. However, if the “opioid crisis” includes multiple substances, the opioid specificity of current prevention and treatment interventions may limit their ability to address the broader problem of polysubstance use involving opioids. To have the maximum impact on this multifaceted crisis, it is important to understand the overlap of opioids with other substances. Overlap of opioids with other substances can include shifts across the lifespan & simultaneous co-use of substances. Use of substances across a broad time frame (i.e., past year or lifetime) is typical for epidemiological studies, which less commonly assess specific co-use patterns within specific drug-using occasions. However, the primary focus of this Perspective is on the issue of simultaneous co-use of an opioid with another substance, which could include nicotine, alcohol, other opioids including prescribed opioids, benzodiazepines (& other sedatives), stimulants including cocaine & amphetamine-related compounds, & other categories.
There are multiple reasons people use other substances with opioids: enhancement of the high (additive or synergistic reward), compensation for undesired effects of one drug by taking another, compensation for negative internal states, or a general predisposition for all substances. The possibility that consuming multiple substances in combination has additive or synergistic pharmacological effects particularly demands study. Fortunately, we are now at a point where advances in research methods allow us to study these kinds of complexities, moving addiction science beyond the typically single-drug models of the past.
In this Perspective, we summarize overlaps of opioid use & addiction with the use of & addiction to other substances from viewpoints of population science & then neuroscience. In each section, we address questions of why nonmedical opioid users also commonly use other drugs, & what are health consequences of simultaneous use of multiple drugs are, including their role in overdose deaths
Population Studies Epidemiological studies dating back at least several decades confirm that persons with OUD are likely to have used multiple substances, not just opioids. The Epidemiologic Catchment Area data from the early 1980s showed that, on average, heroin users consumed 5.0 other illicit substances (out of seven categories assessed & excluding tobacco or alcohol) & users of opioids other than heroin consumed 5.8 others. Results from observational studies of returning Vietnam Veterans and samples of heroin users in Miami & California confirm other drug use as a prominent risk factor for subsequent heroin use & overlapping co-use of heroin with other substances.
More recent studies also have documented that opioid use overlaps with other substances and that OUD often co-occurs with other substance use disorders. A 2012–2013 U.S. general population study found that more than 90% of individuals with OUD used more than two other substances within the same year, & over 25% had at least two other substance use disorders along with OUD. Those with more substance use disorders were more likely to be younger, male, & single and were more likely to have initiated opioid use at an earlier age. Finally, a notable indicator of simultaneous multi-substance use is that the majority of opioid-related overdose deaths involve multiple substances.
While overlap with other substances & substance use disorders is common among those with OUD, the patterns may vary. Recent evidence shows an increasing rate of methamphetamine use among adults in the U.S. admitted to treatment programs for heroin addiction. The implication is that the overlap of opioids with other substances is common but can vary across time, both within an individual & within populations of users.
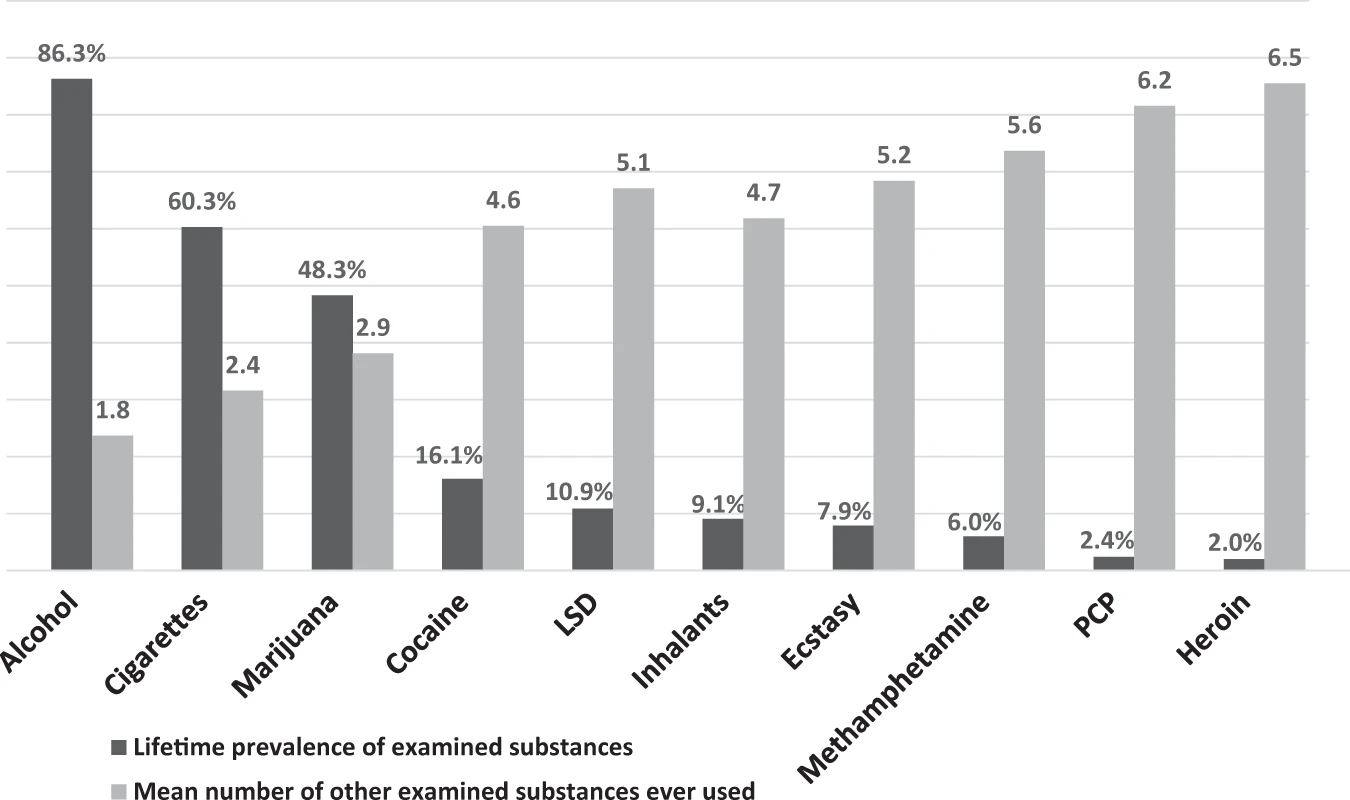
While the focus of this Perspective is on polysubstance use in the context of opioids, it is important to consider that polysubstance use frequently occurs with all recreational drugs, whether their use is legal or illegal. Cigarette smokers are far more likely to drink alcohol than non-smokers. Marijuana users are far more likely to use opioids nonmedically than people who do not use marijuana. This pattern is seen in all ages & drug-using populations. Further, as a general principle, the more widely a drug is used, the higher the percentage of users who do not use other drugs & the less widely used, the more likely a drug is to be used with other drugs. While the reasons for this increasing overlap in substances that are less frequently consumed are not totally clear, some of it may relate to the drug use trajectories where substances are added to one another in a progression. Because less frequently consumed substances are rarely the first used, it is typical that less frequently consumed substances would have a higher degree of overlap over the life course than the more commonly consumed ones. This principle may help explain the high frequency of overlap of heroin use with other drug use & the lesser, but still significant, overlap of prescription opioid misuse (which is much more common than heroin use) with other drug use.